26 May – Beyond the Budget Series

Killian Carroll, Senior Economist
In our previous blog, we looked at recent current spending overruns across government and argued that these reflected not only weak expenditure management, but also bad budgeting and planning. This blog looks at one important example of bad budgeting: health spending.1
Health overruns are often discussed as a failure to control spending during the year. That is part of the story. But some of the problems start earlier, when budgets are set. In health, and especially in hospitals, budgets have repeatedly been set as if the previous year’s actual level of spending did not happen. This means they have implicitly assumed large savings from efficiency or better care models, even though similar savings failed to materialise in previous years.
A large share of the overruns has been driven by health spending
Our previous blog showed that, excluding new cost-of-living measures introduced during the year, total current spending exceeded budgeted amounts by €2 billion (2.6%) in 2023, €3.2 billion (3.8%) in 2024, and €2.4 billion (2.6%) in 2025.
Health accounted for a large share of these overruns. As the chart below shows, health made up more than 40% of total current spending overruns across these years. It accounted for 50% of the overrun in 2023 and 55% in 2024, before falling to 14% in 2025.
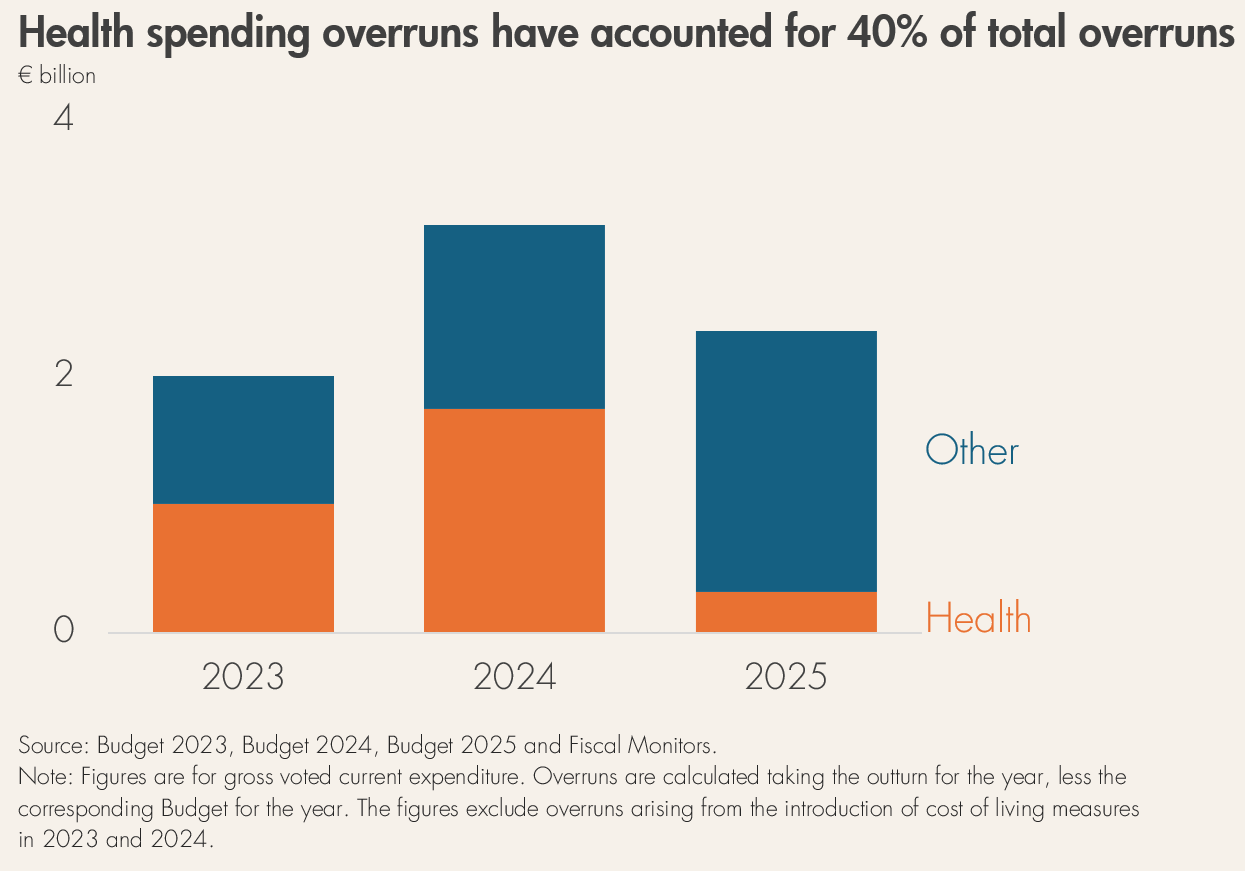
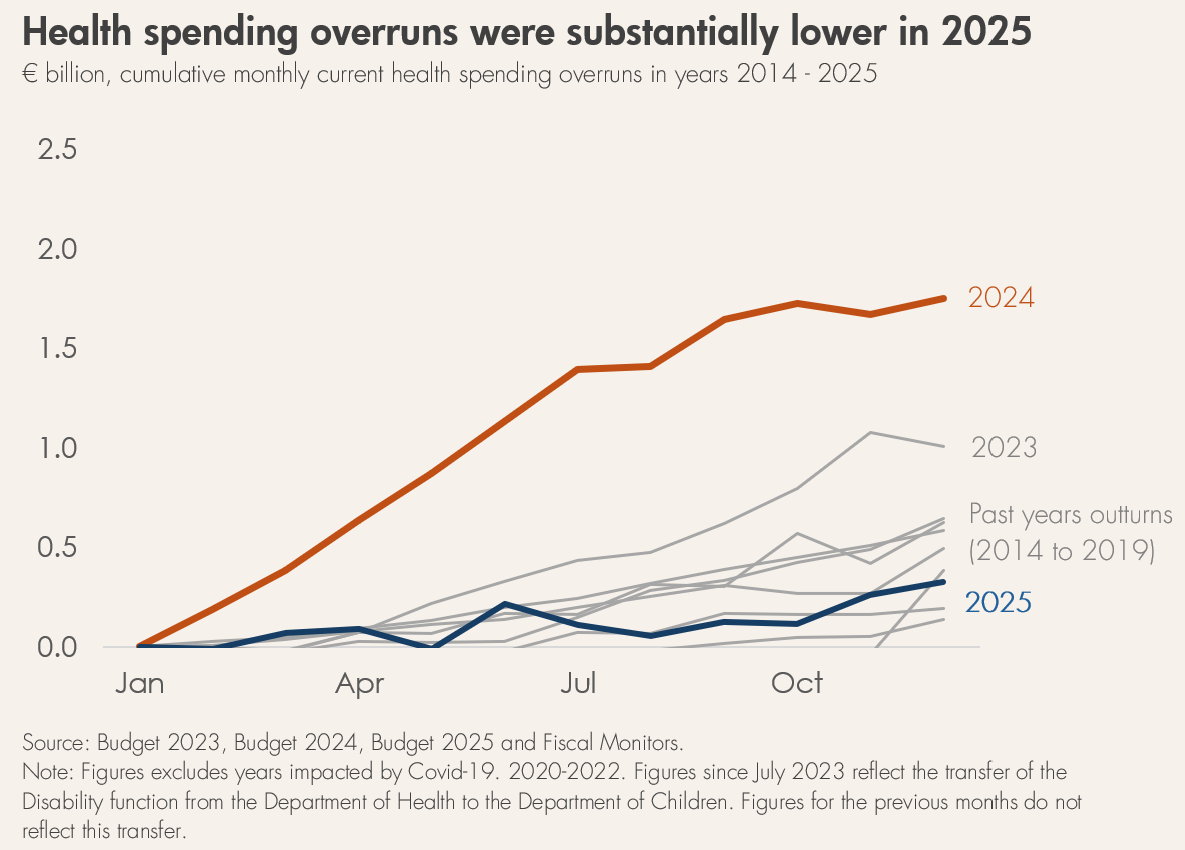
The overrun in 2024 was particularly striking. Health spending exceeded its budget by €1.75 billion (8.1%)—the largest overrun on record.2 Unlike previous years, this overrun was apparent from an early stage.
That prompted one of the first major examples of multiannual budgeting in Ireland: the two-year expenditure agreement announced in the Summer Economic Statement 2024. This provided an additional €2.7 billion for health across the remainder of 2024 and 2025.
That multiannual approach is welcome. It helped put health spending on a more realistic footing and should be repeated, both in health and in other areas of spending. Following the agreement, the 2025 overrun in health was the smallest since 2017.
However, multiannual budgeting alone is not enough. It needs to be based on realistic estimates of the cost of maintaining existing services, given demographic and price pressures.
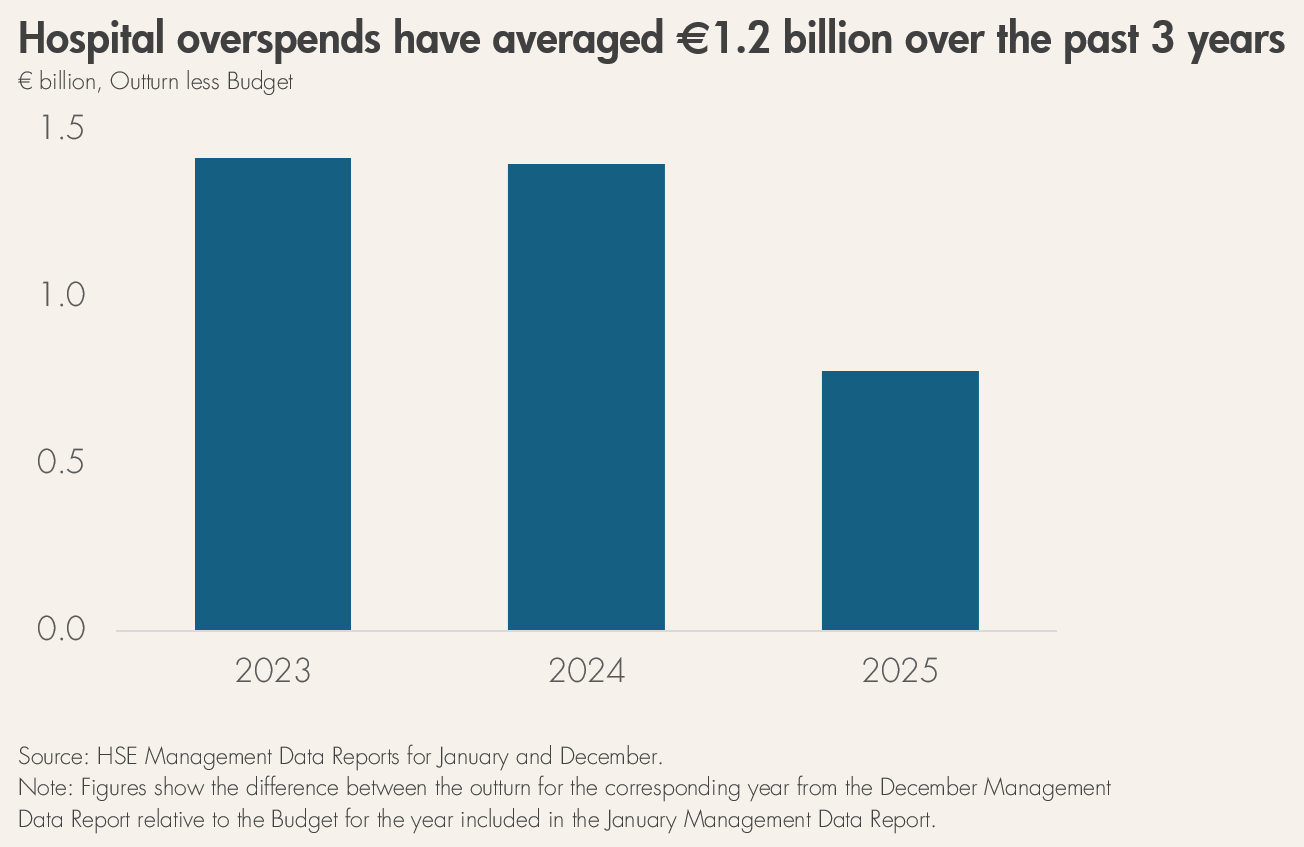
Hospitals show the budgeting problem clearly
A clear example can be seen in hospital spending. Hospitals are the largest area of HSE spending, accounting for an average of 37% of total HSE spending over 2023-2025. Over the past three years, hospital spending has overrun by an average of €1.2 billion a year.
Part of this reflects bad budgeting. The chart below compares each year’s hospital budget with the amount actually spent on hospitals in the previous year. These figures are taken from the HSE Management Data Reports for January of the current year and December of the preceding year.
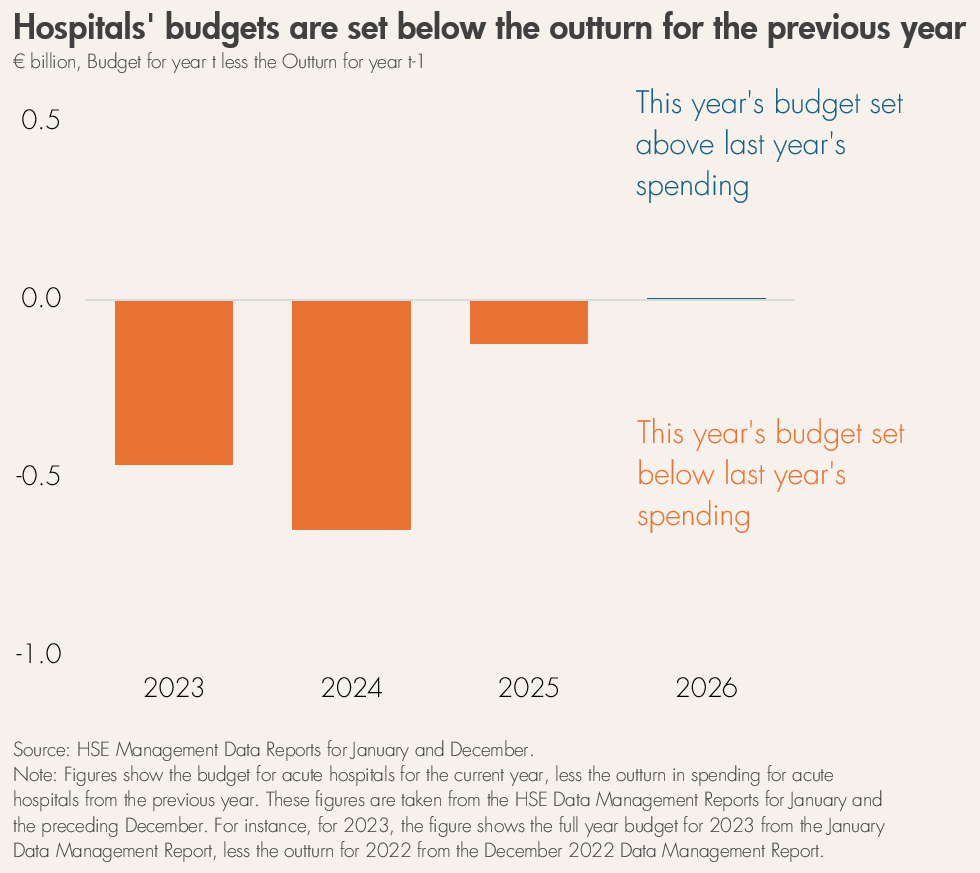
In each year from 2023 to 2025, the budget for hospitals was set below the previous year’s actual level of spending. For example, the 2024 budget for acute hospitals was set €0.6 billion below what was actually spent in 2023.
This is difficult to justify. In the absence of policy changes, the cost of maintaining existing health services would normally be expected to rise from year to year. Staff pay increases, health sector inflation, demographic pressures, and growing demand all tend to push spending upwards.
Setting the budget below the previous year’s actual spending therefore implies sizeable efficiency savings or big reductions in the level of service provided. But the persistent overruns suggest that these savings assumptions were unrealistic. In effect, savings that failed to materialise one year were assumed again the next.
Are the overruns predictable?
There is also a clear relationship between the size of the budgeting gap and the overruns that followed. Among the years shown, 2024 had the largest gap between the hospital budget and previous-year spending, and it also had the largest overrun. The next largest gap was in 2023, which had the next largest overrun. The smallest gap was in 2025, which had the smallest overrun. On average, this gap accounted for around 40% of the hospital overrun in each year.3
This suggests that poor baseline budgeting has played a substantial role in health overruns. The lower overrun in 2025 also shows the potential benefits of a more realistic, multiannual approach.
For this to work, budgets must be based on reliable estimates of current service costs and realistic savings targets. Otherwise, a “soft budget constraint” can return: spending targets aren’t realistic, spending caps are repeatedly loosened, health managers stop seeing them as credible, and efforts to control spending may weaken, leading to more unplanned spending increases.
What will happen in 2026?
The acute hospital budget for 2026 is higher than the actual level of spending in 2025, making it the only year in the past four where this has been the case. But the increase is marginal: just €6 million.
That is unlikely to be enough. Known price pressures, pay increases, demographic change, and demand for services mean that the cost of maintaining existing hospital services is likely to rise substantially. And that is before any new policy measures are implemented. A budget that is only fractionally above last year’s spending still appears to rely on significant savings.
Indeed, we have already seen indications that the HSE is €0.25 billion over budget in the first quarter alone. 4 While it is certain that there will be an overrun, it remains to be seen how large the final overrun will be.
More realistic budgeting is needed
After several years in which large, assumed savings failed to materialise, it is questionable whether budgets should continue to rely on them. Without more realistic budgeting, health spending is likely to overrun again in 2026. How large that overrun becomes will depend on expenditure management during the year.
The opinions expressed and arguments employed in these blogs do not necessarily reflect the official views of the Fiscal Council.
Footnotes
- For a detailed discussion on some of the other main drivers of health overruns, see Casey & Carroll (2021). ↩︎
- Excluding Covid-19 years. ↩︎
- This is the minimum overrun that can be attributed to bad budgeting. With demographic and price pressures, bad budgeting is likely causing a higher share of the hospital budget overrun. The remainder can be attributed to poor expenditure management. ↩︎
- See reporting in the Irish Times on the overspend in Q1 ↩︎